Breast Reconstruction Surgery
Choosing whether to undergo breast reconstruction after a mastectomy is a deeply personal decision, and the range of available options can sometimes feel overwhelming. At Farkas Plastic Surgery, our team is here to provide clear guidance, compassionate support, and honest information at every step. We understand that this is a challenging time, and we strive to make your experience as smooth, comfortable, and reassuring as possible.
The information below can give you an overview of the advanced breast reconstruction options available from our board-certified plastic surgeon, Dr. Jordan P. Farkas, and the treatment process. If questions or concerns arise at any point, we encourage you to reach out to Dr. Farkas or a member of our team. We’re here for you.
Breast Reconstruction At a Glance
- Potential Benefits:
- Restores breast shape and symmetry following mastectomy, helping many patients feel more like themselves and improving overall confidence and quality of life.
- Candidates:
- Women who have undergone or are planning a mastectomy due to breast cancer or other conditions, and who are in good general health with realistic expectations for their outcome.
- Procedure:
- May involve implant-based reconstruction, autologous tissue (flap) techniques, or a combination approach. Surgery can often be performed at the same time as the mastectomy or in a staged manner depending on your treatment plan.
- Recovery:
- Initial recovery varies by technique, but most patients can resume light activities within a few weeks. Full healing and final results should develop gradually over several months as swelling subsides and tissues settle.
- Insurance:
- In many cases, health insurance covers breast reconstruction following mastectomy, including certain revision procedures to improve symmetry or outcomes. Our team assists with pre-certification and claims submission.
- Surgeon:
- Dr. Jordan P. Farkas is certified by the American Board of Plastic Surgery and has extensive experience performing advanced breast reconstruction techniques. Each treatment plan is highly personalized to align with your anatomy, medical needs, and aesthetic goals.
Explore Topics On This Page:
- Diagnosis of Breast Cancer
- Breast Reconstruction Procedures
- Deep Inferior Epigastric Artery Perforator Flap (DIEP Flap) Breast Reconstruction
- Pedicled TRAM Flap Breast Reconstruction
- Prosthetic Implant with Acellular Dermal Matrix Breast Reconstruction
- Delayed vs. Immediate Breast Reconstruction
- Breast Reconstruction Insurance
A Diagnosis of Breast Cancer
Unfortunately, a diagnosis of breast cancer is common and is a traumatic event for every woman and family. For many of these women, treatment with breast conservation surgery (i.e. lumpectomy) may be an option. For others, however, treatment with mastectomy may be the recommendation from the breast surgeons. Although all questions related to your breast cancer care are best-suited for your excellent breast cancer team and surgeons, plastic surgery can be explored as a way to reconstruct the breasts following a mastectomy.
For those who undergo a mastectomy, losing one or both breasts can have a devastating psychological impact on one’s self-image and self-confidence; however, advanced breast reconstructive techniques offer a variety of options for many individuals to restore the appearance of the breasts. Plastic and reconstructive surgeons now have the ability to provide women with a natural-appearing breast shape following their mastectomy. As recently as 25 years ago, options for post-mastectomy breast reconstruction were severely limited. Furthermore, the results of those procedures in use may have been generally unnatural and lacking. Fortunately, advances in plastic surgery made since that time have enabled us to offer both single and double mastectomy patients several excellent options for breast reconstruction.
What Are the Different Types of Breast Reconstruction Procedures?
Procedures for breast reconstruction available today can be done at the same time as the mastectomy, or after waiting a few months to several years. There are, in general, three reconstructive options, each with its own advantages and disadvantages. Our physician will discuss in detail all the reconstructive options available to you. The goal of the consultation is to provide you and your loved ones all the information regarding your reconstructive options so that you may select the breast reconstruction that is best suited for you.
Option 1
The first option, called autologous breast reconstruction involves reconstructing a breast with the patient’s own tissues. These tissues are generally taken from the abdomen, the back, or the thighs, with the abdomen being the most common (the “DIEP flap”).
The main advantage of autologous breast reconstruction is that because the breast is reconstructed with the patient’s own tissues, it is the most “natural” reconstruction as these tissues will heal and grow with the patient, and require no maintenance or upkeep.
The main disadvantage of autologous breast reconstruction techniques are the donor site changes; however, in some cases, patients may find they are actually advantageous, such as when tissue is taken from the abdomen or medial thigh.
In recent years, there have been dramatic technical advances in autologous breast reconstruction, which is considered by many to be the “gold standard” of breast reconstruction. Advances in microvascular surgery, such as the DIEP flap technique, have made it possible to transfer the necessary tissue with minimal trauma to the donor site. This has resulted in dramatically reduced donor site problems without compromising the outcome of the breast reconstruction. Furthermore, these technological advances have made the option of autologous breast reconstruction a reality for patients who previously were not considered good candidates.
However, infrequent issues, such as pseudo-hernias (aka abdominal bulge), fat necrosis, partial flap losses, numbness, and weakness may be a long-standing complication of autologous reconstruction. Furthermore, autologous breast reconstruction procedures generally take slightly longer than other implant-based options on account of the technical aspect of the surgery. Lastly and most importantly, unfortunately not every patient is a candidate for an autologous breast reconstruction. Factors such as body habitus, previous surgeries, smoking history, and co-existing medical conditions may be prohibitive. Dr. Farkas will discuss all of this information with you in great detail at your in-office consultation. The autologous reconstruction can either be performed at the time of the mastectomy or, depending on the need for post-mastectomy radiation, in a “delayed” fashion. If post-mastectomy radiation is planned, then usually a tissue expander would be placed at the time of the mastectomy and act as a spacer until the autologous reconstruction is performed. It is generally delayed six months after the completion of the radiation therapy to allow for adequate healing to the soft tissues and chest.
Option 2
The second excellent option for breast reconstruction is an implant-based breast reconstruction. This technique uses breast implants, either silicone or saline, to reconstruct the breast mound. This can be performed as either a single-stage (a permanent implant placed at the same time as the mastectomy) or two-stage procedure (using an expander followed by implant insertion), depending on your breast size and shape. The tissue expander or implant can be placed either above the pectoral muscle (pre-pectoral) or under the muscle (submuscular).
Dr. Farkas will discuss the benefits and disadvantages of each of these types of reconstruction in detail. Prosthetic breast reconstruction techniques spare the patient the loss of donor site tissue as well as donor-site scarring. It is currently recommended by the FDA to have the implants evaluated for possible exchange 10-15 years after placement. If a tissue expander if placed, the patient will have weekly expansions that usually begin two weeks following the mastectomy until the desired volume is achieved. Once the volume of the expanded pocket is deemed adequate the soft tissue heals for approximately 4-6 weeks and then the permanent implant is exchanged at a second operation.
Option 3
The third option for breast reconstruction uses a combination of the first two options. This option involves the transfer of the patient’s own tissues (usually from the back or abdomen) in combination with the insertion of a tissue expander or implant. This option encompasses both the advantages and disadvantages of autologous and prosthetic breast reconstruction techniques. It is generally used when an implant reconstruction is planned but there is a lack of healthy, pliable soft tissue at the mastectomy site or insufficient donor soft tissue volume.
Deep Inferior Epigastric Artery Perforator Flap (DIEP Flap) Breast Reconstruction
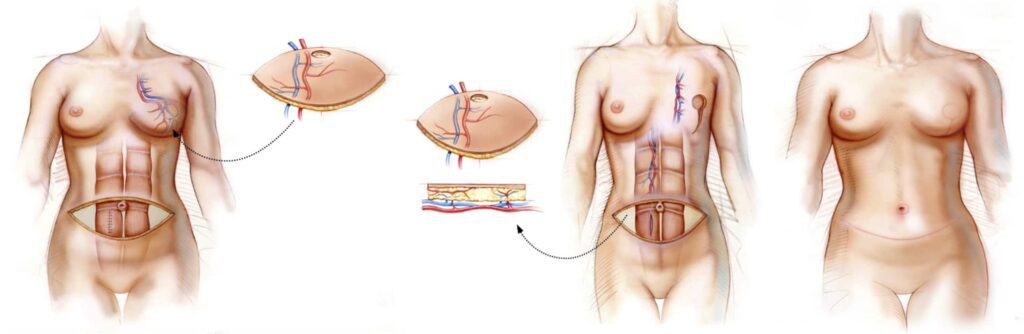
The deep inferior epigastric artery perforator flap is a newer abdomen-based reconstruction option for select patients that over the past 15 years has supplanted the free transverse rectus abdominal muscle (TRAM) flap. The DIEP flap uses the abdominal skin and fat only avoiding the sacrifice of the rectus abdominus muscles (6-pack muscles), improving the post-operative recovery, often producing less pain, and preventing any future abdominal wall weakness.
The procedure is very similar to the free TRAM flap with disconnecting the arteries and veins in the groin and reconnecting them microscopically to an artery and vein in the chest. However, the arteries and veins are dissected free from the rectus abdominus muscle.
Post-operatively there is an incision along the inferior portion of the abdomen from hip to hip and around the belly button similar to the scars of an abdominoplasty (tummy tuck). Depending on the type of mastectomy that was performed, the incisions on the breast are generally the same incisions used to place the flap in the chest.
Patients who have had prior abdominal surgeries may still be candidates for the reconstruction, and we get a pre-operative MRA of the abdomen to use as a map of the blood vessels of the abdomen to ensure that there is adequate vascular supply for the flap procedure.
Post-operatively, patients are monitored in the intensive care unit for flap monitoring purposes only for 24-48 hrs and usually have a 3-5 day hospital stay.
Pedicled TRAM Flap Breast Reconstruction
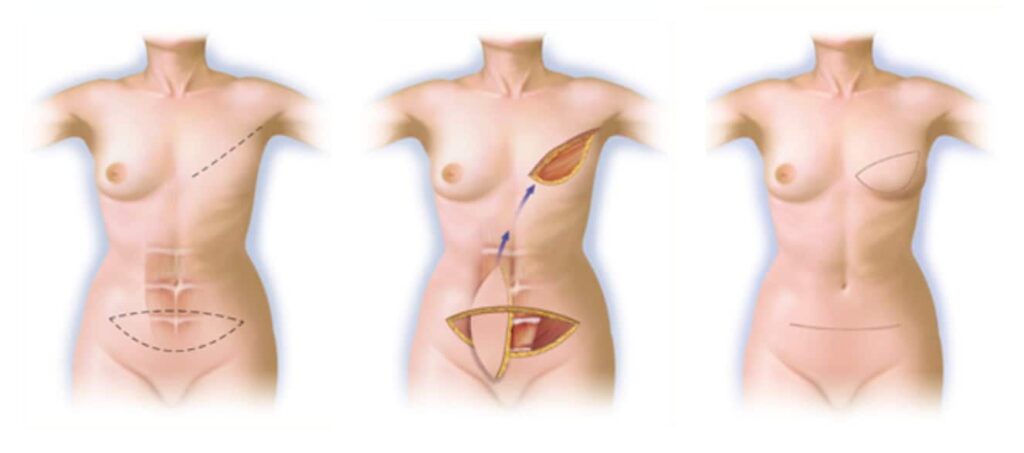
A football shaped piece of abdominal skin and subcutaneous tissue is elevated (the same type of tissue that is used for the DIEP flap technique noted above), and shaped to recreate a breast mound. This tissue is kept attached to the underlying rectus abdominis muscle, which contains its blood supply (or “pedicle”), and tunneled through the mastectomy site.
Prosthetic Implant with Acellular Dermal Matrix Breast Reconstruction
Traditionally with prosthetic implant breast reconstruction, a balloon tissue expander is inserted into the mastectomy site under the pectoralis muscle to create a pocket where the implant will ultimately lie, and then expanded weekly over a 2-3 month period prior to exchanging it for a permanent saline or silicone breast implant. Acellular dermal matrix is used to create either an “instant pocket” by using the tissue at the lower aspect of the breast, acting as a sling or hammock for the implant or, as with a more recent innovation, placing the implant over the muscle as a natural breast and creating a pocket covering the entire implant or expander with the tissue, avoiding the need to release and cut the muscle. The newer pre-pectoral technique has dramatically decreased the recovery time and recuperation associated with implant-based reconstruction and options will be discussed at your consultation. Depending on the size and shape of your breast you may be a candidate to have the permanent implant placed at the time of your mastectomy, either above or below the muscle, sometimes referred to as a direct-to-implant procedure. This will be discussed at the time of your in-office consultation.
If an expander is placed it will be expanded by an injection of air, which is performed weekly at the doctor’s office. After weeks of expansion (usually 6 – 10 weeks), when the pocket is deemed large enough, the patient is taken back to the operating room approximately 4 weeks later to replace the expander with a permanent implant, which may be made of either saline or silicone.
Delayed vs. Immediate Breast Reconstruction
One of the most important decisions in your reconstruction journey is determining the timing of your procedure. Breast reconstruction can typically be performed either immediately at the time of mastectomy or delayed until a later date, and each option offers distinct advantages.
Immediate breast reconstruction is performed during the same operation as the mastectomy. This approach allows patients to wake up with the beginnings of a reconstructed breast already in place, which can be emotionally beneficial for many women. It may also reduce the total number of surgeries and help preserve more of the natural breast skin, which may lead to more refined aesthetic results. However, immediate reconstruction is not always recommended for every patient, particularly if post-mastectomy radiation therapy is anticipated, as radiation can affect healing and final outcomes.
Delayed breast reconstruction, on the other hand, is performed after the mastectomy site has fully healed, sometimes months or even years later. This approach is often preferred when additional cancer treatments such as radiation are required, or when patients wish to take more time to consider their reconstructive options. While it may involve additional procedures and a longer overall timeline, delayed reconstruction allows for greater flexibility in surgical planning once the body has recovered from initial cancer treatments.
Ultimately, the choice between immediate and delayed reconstruction depends on a variety of factors, including your overall health, cancer treatment plan, lifestyle, and personal preferences. Dr. Farkas works closely with each patient and their oncology team to develop a thoughtful, customized approach that prioritizes both safety and long-term results.
Does Insurance Cover Breast Reconstruction?
For patients undergoing mastectomy for breast cancer, health insurance will generally cover a portion of the procedure cost. Although Farkas Plastic Surgery is out-of-network with all insurance companies and managed care plans (except Medicare®), we do accept most types of insurance payments and, as a courtesy to our patients, we will submit the pre-certification and claims directly to the insurance company on our patients’ behalf.
In some cases there could be out-of-pocket expenses relative to your insurance plan. We want to make the payment process as convenient as possible for all of our patients, which is why we accept numerous payment methods and work with reputable third-party healthcare financing companies. A variety of financing options available through these companies enable qualified applicants to pay for their treatment over time instead of all at once.
“Dr Farkas and his entire staff were amazing during before and after my surgery. I was comfortable as he answered any questions I had honestly and guided me through the process. My recovery has been easy and my healing is great and I am so happy with my results! I would highly recommend him to anyone considering surgery.”
If you have questions about breast reconstruction, or if you would like to schedule a consultation with our plastic surgeon to discuss your options, please don’t hesitate to contact our office.
